The patient returned for a follow-up approximately one month after receiving the custom orthotics that we fabricated in our office. I asked if they had been effective; was she able to return to her typical work days and walking for exercise without metatarsal pain. She stated that she was able to do everything except walk barefoot.
She said "That still hurts. Am I going to need surgery?"
When I attempted to review the nature of her foot issue and why walking for long periods without her shoes and inserts would likely flare it up, the patient told me that she was confused. Since I had last seen her, she had sought a third and fourth opinion (in addition to mine and the podiatrist who referred her to our office).
Her concern went something like this:
"The first foot doctor said my foot pain was from the middle metatarsal bones dropping down, which he saw on the X ray. You said that my walking was off and the insert would provide better spacing. The second podiatrist took and MRI and said that it was from bursa swelling and inflammation. The third doctor thought I was doing well but would need new shoes. So what's the problem here?"
My task then was to show her that everyone she visited had independently reached the same conclusion but focused on different labels.
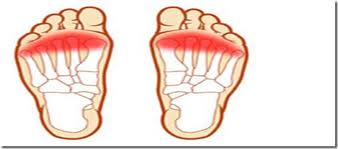
I explained that when the metatarsal bones drop, the foot loses the transverse/across the foot arch and the bones get repeatedly jammed together, which irritates the bursa and tendon sheaths in that area. Displacement of the natural cushion (plantar fat pad) causes high pressure right under the balls of the feet.
"We're all talking about the same thing."
Call it a dropped metatarsal, metatarsalgia, forefoot bursitis, gait dysfunction, or neuroma. The real question is "What are you going to do about it?" Even surgery usually requires some other intervention to achieve a favorable long-term outcome.
In this case, we focused on having the patient improve her gait pattern to include less turning out of the foot and torquing off her 4th and 5th toes. Some foot strengthening, hip and ankle mobility work, and gait training were critical for her to make and successfully retain those changes. The custom insert with a semi rigid shell and specifically placed metatarsal pad would provide structural support to maintain the transverse arch across the mid- and forefoot.
We also had to address her leg length discrepancy - not a few millimeters of no big deal, but a glaring problem that any layperson would say that she was jamming her one foot into the ground. Lastly, at the advice of the fourth specialist, she did purchase a quality shoe that provided more toe room and greater support to help maintain the entire foot in a neutral position rather than folding and twisting under the weight of her body.
The gait training, the exercises, the custom orthotic with heel lift, and the shoes - none of those things alone would have been sufficient to circumvent the chronic condition. But taken together, her current situation and long term prognosis seems favorable.
- - - - -
No comments:
Post a Comment